Popularly known as a “boob job”, breast augmentation remains the most in-demand cosmetic surgical procedure today. According to International Society of Aesthetic Plastic Surgery (ISAPS), there were 1,677,319 breast augmentation procedures recorded worldwide in 2017. Based on that number, the use of saline implants increased by 13 percent, [^1] with more than 8000 performed on young girls below 20 years old in the US alone. [^2]
Introduction to Breast Augmentation
Many women around the world are unhappy with their breast size, and are willing to go to great lengths to achieve their ideal size and shape. While there are alternative, non-invasive approaches such as taking pills, or using contraptions that claim to increase your cup size from A to C, only elective surgery such as breast augmentation, or augmentation mammaplasty, is proven to be the most effective at this task.
With continuously growing numbers, it seems that breast augmentation is not going to wane in popularity any time soon.
History of breast augmentation and implant use
The use of implants to increase breast size came to be in the early 60s. [^3] They were made of silicone casing and filled with either silicone gel, or saline solution. However, they weren’t as popular at the time as they are now. This cosmetic procedure involving major surgery only started to fully take off in the 80s, with over 1 million women having subjected themselves to breast augmentation by 1990.
Vincenz Czerny, a German surgeon often referred to as the “father of cosmetic breast surgery”, was first known to attempt the enlargement of a woman’s breast in 1895 by implanting it with lumbar lipoma, which is a fatty lump from the abdominal segment of the torso. [^4] During that time, the surgery was not performed for vanity reasons, instead, the breasts of the patient needed reconstruction after the removal of a benign tumor.
This corrective procedure turned out to be a seminal moment in breast augmentation. Other surgeons soon followed, but were unsuccessful with their disastrous injections of paraffin and implantation of polyvinyl alcohol sponge. [^4] Nonetheless, many continued to use paraffin injections in augmenting breasts of women up until 1914. [^5]
After World War II, some Japanese women started injecting themselves with stolen industrial-grade silicone, which were intended for military purposes. As such, complications that arose from paraffin injections were repeated with silicone use, especially with the toxic additives and impurities given their preparations that include cobra venom and olive oil. [^5]
The problem with liquid silicone is its instability; it cannot maintain its form in the injected site. It tends to form granulomas, which can migrate into surrounding areas of the body. Worse, it can cause necrosis or cell death. [^6]
As breast augmentation continued to evolve, first gen breast implants consisted of solid materials such as Teflon and Ivalon sponge during the late fifties. All patients who received this type of implantation developed abnormally firm breasts and experienced a 25-percent loss in breast volume, which resulted in distortion of the breast. [^7] Other complications included are bacterial infection, local tissue reaction, implant erosion, and general discomfort. [^8]
With the development of medical grade silicone in 1960 by Dow Corning Corporation, [^9] the silicone implant was engineered by doctors Frank Gerow and Thomas Cronin using a thick shell made of silicone elastomer, and filled with a viscous silicone gel. [^10] A dog named Esmeralda was the first recipient of this type of implant, followed by Timmie Jean Lindsey, a Texan factory worker and divorced mother of 6. She became the first human to have undergone breast augmentation using a silicone implant in 1962.
Saline implants succeeded the silicone towards the end of 1960. The first ones using inflatable types were reported in France in 1965. [^11] Instead of just a pre-filled implant, these options allow empty casings to be filled with saltwater while already placed in the body.
The silicone implant continued to be used for breast augmentation without the approval from the FDA for many decades since its inception. Breast implant manufacturers were not required to prove the safety of their products until 1991. This was when it has been questioned and brought to light, with Mariann Hopkins winning a 7.3 million-lawsuit against Dow Corning Corp. for her ruptured breast implants.
In the meantime, saline implants remained untouched in the face of the implant safety controversy, gaining the approval of the FDA in 2000. The silicone implant followed many years later in 2006.
In 2011, the FDA issued a safety communication regarding the possible association of breast implants and large cell lymphoma. [^12] This was also supported by the WHO, several professional organizations and regulatory bodies. Notwithstanding, silicone and saline implants remain viable options for those looking at surgical breast augmentation.
Breast implants should not be considered as devices for life. They may require replacement or removal at any given time. However, Timmie Jean seems to have prolonged hers. During her 2012 BBC interview, she shared that 50 years later, she still had her implants at the time, and treasures them as an important piece of history. This might dispel some doubts about the use of silicone implants that are constantly deemed as unsafe by others.
Reminders about breast augmentation
While women are having their breasts done for a myriad of reasons, may it be aesthetics, corrective, or reconstruction, breast augmentation should be a matter of personal decision. Ultimately, a woman should be doing it for herself, not because her partner or anyone wants her to, or to fit a cookie-cutter image of perfection.
Breast augmentation in a nutshell
Implantation is the most common breast augmentation method which allows you to choose the type and size of implant, its placement, location of the incision, among other things. Silicone gel is often the implant filling of choice of both doctors and patients, which provides a natural feel and look of a real breast tissue.
On the other hand, saline implants are another option which can be used in younger women with just a small incision. Plus, they are cheaper compared to the silicone implants.
The procedure normally takes up to two hours and best done under general anesthesia. It begins with an incision, followed by the placement of the implant. Basic recovery is expected after a day, and the patient may resume working as early as within 3 days. However, this may vary among individuals.
Although breast implants can last long, with a median lifespan estimated at 16.4 years, [^13], you cannot depend on them to stay forever in your body. For as long as a woman has them, she will most probably have another surgery either for replacement or removal. [^14]
Breast implant types
Saline-filled breast implants
Introduced in 1965, saline implants are utilized to increase breast size, which are made of a silicone outer shell and salt water filling. [^14] They come pre-filled, or filled according to desired volume after insertion of their shell in the body.
These implants were originally marketed as a softer implant, which therefore became an alternative to those who have experienced capsular contracture from a silicone implantation. [^15]. As such, they are often used in revision breast surgeries.

Advantages of saline implants:
- Saline implants can be inserted into the breasts using a smaller incision.
- Saline implants have better upper fullness and projection, which can create that “Baywatch look”.
- Saline implants are FDA-approved for use in younger patients who are at least 18 years old. Breast reconstruction using these implants in women is allowed at any age.
- Certain saline implants are adjustable after the operation in order to achieve better size and symmetry.
- In case of an implant rupture, leaking saltwater from the deflated implant will be absorbed by the body without posing health risks to the individual.
- Implant rupture is easier to detect with saline implants.
- Saline implants are cheaper compared to silicone implants.
Disadvantages of saline implants:
- Saline implants may look visible on the external, especially for women with thinner skin, which can increase their chances to ripple.
- Saline implants have a higher risk of leaking.
- Saline implants feel firmer than natural breast tissue.
- Saline implants are heavier, which may contribute to premature sagging.
Silicone gel implants
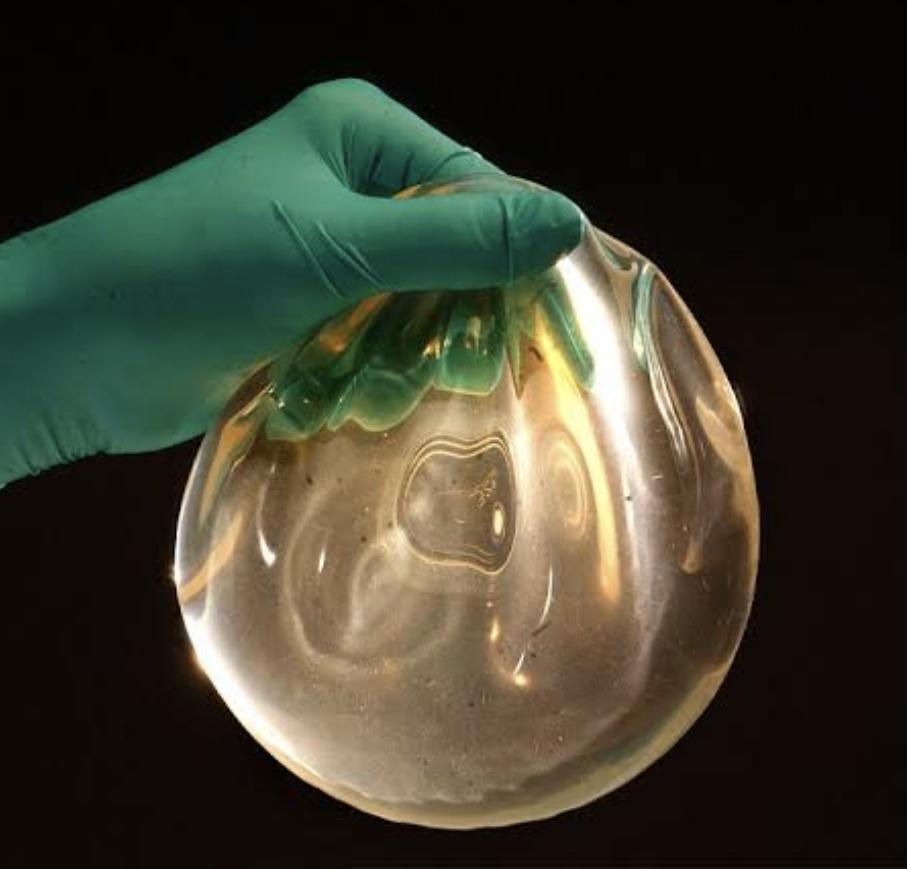
Silicone implants are a highly popular choice for women undergoing breast enhancement. These are silicone shells filled with highly viscous silicone gel. Silicone gel is an inactive polymer with its bonded molecules and has no known human allergies or reactions. [^16] This allows such implants to recreate the natural look and feel of genuine breasts.
Silicone implants are approved for use in women over 21 years old, younger when performed for reconstructive purposes such as those with pre-existing medical, or congenital conditions.
There are currently two types of silicone implants, namely: regular silicone and highly cohesive silicone gel. The highly cohesive silicone gel implants, or gummy bear implants have thicker silicone gel filling than the regular silicone implants. This type of implant holds their shape and does not deform as much as the conventional kind. It is gaining popularity given its improved characteristics and satisfactory results.
Advantages of silicone implants:
- Silicone implants have a softer, more natural feel than saline implants.
- Silicone implants have less occurrences of rippling.
- Silicone gummy bear implants have lower rates of implant rupture and capsular contracture.
- Silicone gummy bear implants are able to preserve their shape longer, giving enhanced projection.
- Silicone gummy bear implants are less prone to malposition.
Disadvantages of silicone implants:
- Silicone implants require larger incisions to accommodate the pre-filled silicone shells.
- Implant rupture can go undetected for a long time with silicone implants as they don’t easily collapse, which make them difficult to discover.
- Shaped silicone implants may have an increased risk for malrotation unlike round implants.
Structured saline breast implants
The structured breast implant is considered a third implant because of its use of a different type of technology. [^17] Approved by the FDA in 2014, this implant has a round shape that also uses saline solution as its filling. The difference lies in its interior structure that targets to achieve the combined benefits of silicone and saline breast implants.
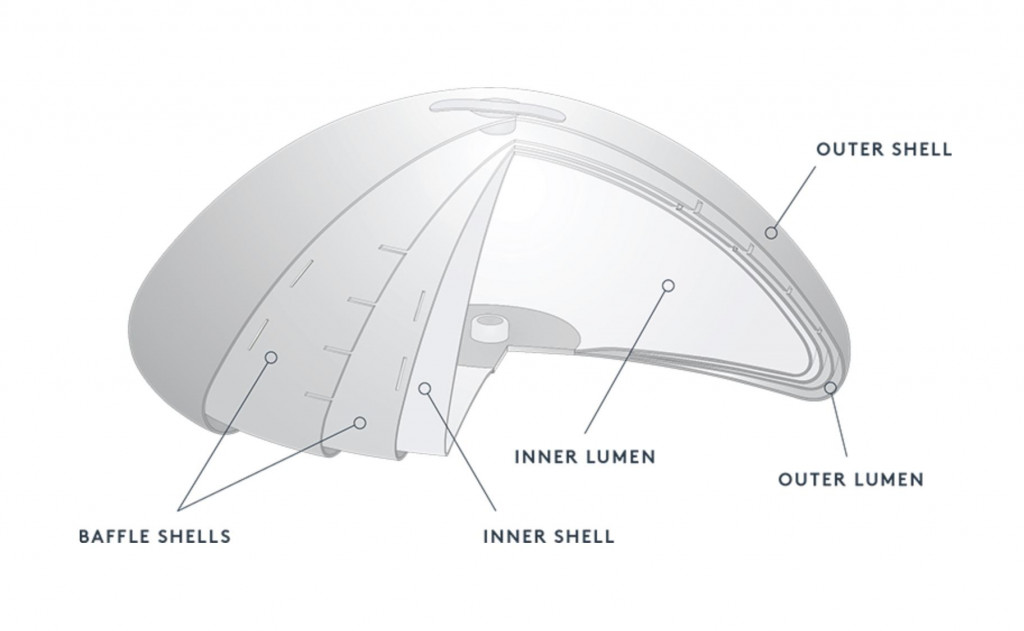
Branded as Ideal implant, this device boasts of having the safety you get from its saltwater solution and at the same time, providing the natural feel which one typically finds in a silicone type. It has two chambers, the one at the rear has a fixed volume while the floating structure may have several baffle shells. These baffles have slits that allow movement of saltwater to and from, but in a controlled way.
The low edge design provides a better contour while giving the projection of a high profile implant. Given its internal structure, the shell has more support which decreases collapse of the upper form when in the upright position, and diminishes the incidence of wrinkling that is common in regular saline implants. [^17]
Advantages of structured implants:
- Structured implant uses saline solution, yet it provides a more natural feel than a regular saline breast implant.
- Structured saline implants have no risk of overfilling.
- Structured implants have minimized rippling compared to typical saline implants.
- Structured implants have less incidences of rupture and capsular contracture.
- Implant rupture remains easily detectable in structured implants compared to silicone implants.
Disadvantages of structured implants:
- Structured implants are slightly firmer to the touch than silicone implants.
- Structure implants provide a single style of projection that is similar to a high profile implant.
Other breast augmentation procedures and supplemental techniques
1) Temporary saline injections (InstaBreast)
As mentioned, breast augmentation should be decided by the patient for herself. There are times when a person wanting breast enhancement cannot fully commit to the surgery just yet. She can undergo a trial period instead by using a new technique named InstaBreast.
InstaBreast was developed by Dr. Norman Rowe, a cosmetic surgeon and diplomate of American Board of Plastic Surgery. It is loosely referred to as vacation breasts, and is completely implant-free. It is a minimally invasive method that temporarily adds volume and fullness to the breast via saline injections.
This device lasts for an estimated 24 hours, after which, the breasts would return to their original size. This is performed for less than 20 minutes and has zero downtime. Clients can resume their work or activity immediately after.
With each session priced from $2,500 to $3,500, InstaBreast is able to provide would-be breast implant patients a more accurate representation of what they will get when they eventually decide to have breast implants. According to Dr Rowe, InstaBreast has a high conversion rate such that, around 75 percent of those who used InstaBreast actually proceeded with the breast augmentation surgery.
2) Breast lipofilling (Fat transfer)
This reconstructive technique is usually mistaken as non-surgical because it can be done using local anesthesia. Autologous fat transfer or fat grafting, is the harvesting of fat from one’s own body part such as arms, thighs, back, or flank) through liposuction. It is then subjected to a purification treatment, before it is injected into the breasts.
The said purification on the harvested fat may involve using insulin for better cell survival, [^18] or it can be further refined via centrifugation in a closed system. [^19] The latter process is able to discard aqueous fat layers, leaving only concentrated viable fat cells in the end product. [^20]
Fat transfer provides a low risk option for some patients, especially those who do not like implants, and would prefer to use excess fat in her body instead. Also, women who are looking at a relatively mild to moderate increase in breast size, will benefit from this procedure by achieving more natural results.
If your goal is to increase your breast to at least 2 cup sizes, or you have noticeable sagging of the breasts, this procedure will not be a good fit for you. You will be better off getting breast implants instead.
Aside from the natural enhanced look, one of the bonus benefits you will get from fat transfer is spot reduction. For instance, you can choose to source the fat from the bulge in your tummy, which many would like to get rid of.
With fat grafting, you can reshape not just your breasts, but practically your whole body as well. Another advantage of fat transfer is its small incision. It leaves almost no scar on both the harvested area and the injection site.
While this method may be less invasive than implant surgery, it is not without risk. Some of its possible complications include infection, cyst formation, necrosis, and fat loss. Cysts may also form as a result of hardening of the injected fat.
Centrifugation of harvested fat is usually performed before injection. This procedure is expected to reduce the side effect of fat loss, [^21] although other studies suggest that it does not do anything to improve fat cell survival. [^22]
Often, injected fat can disappear from the breasts as it is reabsorbed by the body. This may lead to the dismal results of uneven breast sizes, which would consequently entail revision surgeries. As such, cost efficiency of fat transfer is low, considering it is a more expensive option than breast implants.
3) Keller funnel
Named after its developer Dr. Kevin Keller, a board-certified plastic surgeon, the Keller Funnel is a disposable device which aids in insertion of silicone gel implants instead of manually placing them by hand. It uses smaller incisions in the breast pockets as a result. [^23] It is designed to minimize stress on the breast implant.
The device resembles a pastry bag down to its tip. It is made of polymeric vinyl cut to the size of the implant and placed one centimeter into the created breast pocket. The implant is removed from its packaging and poured into the slippery interior of the funnel. This makes for easy transfer, thereby eliminating direct hand and skin contact with the implant. [^24]

While the Keller funnel is not a prerequisite for breast implant surgery, it promotes safer implant handling, decreasing risk of contamination by twenty-seven fold. [^25] As concluded in one study, the use of a Keller funnel can significantly lessen the risk of capsular contracture, [^26] which is one of the possible complications of using silicone implants during breast augmentation.
The Keller funnel facilitates delivery of the breast implant than without it, hence a shorter operating procedure than usual ensues, which can take 30 minutes at its fastest.
With the smaller incision required, it promotes quicker healing and reduced pain post surgery. Meanwhile, the cost of this device is less than $150, which is often incorporated in the breast augmentation quotation provided to the patient. But, you will find that there are providers who are able to absorb this cost.
4) Breast tissue expander in breast reconstruction
Breast tissue expansion is a process where the remaining skin on the chest and its surrounding soft tissues are stretched to accommodate a breast implant. This procedure is usually recommended for breast reconstruction following a mastectomy, which is the partial or complete removal of the breasts in order to treat breast cancer.
Once the breast tissue and fat are removed, it can leave a deformity in the patient. [^27] Instead of wearing an external prosthesis to fill in the missing part of the chest, breast reconstruction is almost always the next step. It can be performed right after a mastectomy, or much later.
An empty implant that is much like a deflated balloon, is inserted into the new breast pocket and inflated with saline solution. This stretches the size of the skin and prevents contraction of the wound from the mastectomy. [^28]
The stretching of the skin may feel uncomfortable for a moment, but this procedure does have a low complication rate, and will not interfere with the cancer treatment of the patient. This expander will remain temporarily in the breast pocket from a few weeks to several months [^29] before being replaced by a permanent implant, or harvested autologous fat from another part of the body.
Similar to actual breast implants, tissue expanders come in textured versions as well as they can minimize capsular contracture and migration. [^30] As such, the tissue expander will not move away from the tight skin area where the half of the preserved breast skin envelope is. [^31] This also allows the patient to maintain a good definition on the inframammary line.
Other advantages of using tissue expanders preceding breast augmentation include minimized site damage and salvaged skin tissue flaps, which will prove useful in the following breast reconstruction. [^32]
5) Breast augmentation with lift
We know that breast implants provide an improved projection on the chest, which can already create a “lifted look” in the process. [^33] Nonetheless, a separate breast lift procedure can also be performed in conjunction with mammaplasty. [^34]
Mastopexy or breast lift, is recommended for women with sagging concerns brought about by age, pregnancy, weight loss and genetics. This way, the breasts do not only increase in cup size, but also defy gravity so to speak with its right elevation. The lift enables breast implants to retain their shape as well as their height in the body.
Aside from sagging breasts, those who lack fullness in the top chest region and possess a tuberous breast can benefit from a breast lift, too. This procedure is a great way to maximize your breast implant surgery. Breast lift includes moving the areola and nipple, plus elimination of excess skin which can result in “perkier” breasts.
Breast lift surgery is performed as an outpatient procedure using local or general sedation, and would typically take two hours or less. When done alongside breast implantation, the implants are typically placed first, followed by the mastopexy procedure. The proportions and appearance of the breast, nipple, and implant are reassessed before completing the surgery. [^33]
Patients are expected to feel some type of soreness and swelling post surgery while the breasts are either bandaged, or secured by a surgical bra. Full recovery in terms of being able to wear an underwire bra, or doing one’s regular exercise routine can be achieved in about two months.
With proper care, a woman who has undergone a breast lift alongside breast augmentation may deter the sagging of her breasts for many years to come. It must be noted however, that weight gain or pregnancy can affect your post surgery results. In any case, breast lift is a great supplemental procedure for one’s breast enhancements using either silicone or saline implants.
6) MTF breast augmentation
Also known as MTF top surgery, Male-To-Female breast augmentation is a surgery performed in order to transform the male chest into female breast form. The shape and size can be changed dramatically with the use of breast implants.
The MTF surgery is often the next step in the transition of transgender women, especially when hormone treatments are unable to provide their targeted goals, particularly with their breast development.
The same breast implant procedure and options apply to both cisgender and transgender women. It involves similar surgical techniques and decision-making calls. However, it has been observed that trans women require wider implants than a typical cisgender female. This is to avoid a large gap between the breasts.
Another issue that is common with trans women is the insufficiency of chest skin to accommodate a large cup breast size. Basically, a male chest anatomy is smaller and more lateral compared to the structure of a genetically female.
A successful MTF top surgery does not only boost the female appearance of transgender women, but also enhances her self-esteem by matching her new body to her true identity. [^35] But this is not an option for every transgender female just as it is not for all cisgender women.
There are qualifications one must meet such as being above 18 years old, having a recorded gender dysphoria history, among other things. Those who qualify and proceed with the breast augmentation surgery have an overwhelming improvement in their psychological well-being following the procedure. [^36]
Breast Implant Size and Dimensions
Women may have their own preferences as far as what their breast implant size should be. While there are those who want to go several cups bigger from their original size, many would also prefer breast augmentation results that are natural looking, which could also be a matter of opinion. What others think your size should be, may not be the same as how you would like them.
Here are questions to ask yourself with regard to achieving the right implant dimensions for you.
- Do I like my breasts to look natural, somewhat enhanced, or noticeably larger?
- Will my breast implants affect the way I live my life, such as my daily exercise routine and other physically strenuous activities?
- How will my new breasts impact my clothing choices?
- Will my breast implants look good for my age?
- Will my back problems worsen when I decide to go for bigger breast implants?
- Will my breast implants affect my diet and health?
- What if my breast implants have rippling issues?
- Will large breast implants require me to have a breast lift later on?
- Will I be happy for a long time with the implant size I will choose?
- Will my implant size accommodate any weight loss or gain in the future, such that my breasts won’t be too big?
- Will having bigger breasts be harmonious to the rest of my body proportions?
There are three key dimensions pertaining to round breast implants and they are: diameter, projection, and volume. The diameter usually remains constant regardless of size, while the projection varies from low to high.
A low profile implant is somewhat flat, moderate has a noticeable projection, and high profile has the most projection. The volume is measured in cubic centimeters or ccs. The average implant size is from 250cc to 350cc, which would provide you with a full C cup breast size. [^40] Other surgeons allow up to 400cc implants as the maximum size. [^41]
You might think that your bra size is a good point of reference but, you must know that it has no outright conversion in implant size. On the contrary, bra sizing may underestimate implant volumes. [^37] Determining the “right” implant size should be done after careful planning and shared decision-making between the patient’s wishes and the doctor’s assessment. [^38]
When the desires of the patient contradict what the doctor thinks, further consultation is recommended as well as the need to educate the individual seeking breast augmentation. The clearer the expectations of the client are, the more achievable the goals can be.
Generally, women tend to prefer larger breasts while the more mature women are looking at a modest size. Based on many designs, women’s clothes are fitted for the C-cup breast size. Breasts with larger implants can make a woman feel confident and sexy in swimsuits and lingerie, but they can also be limiting to certain types of clothing they can wear without issue.
If you are the athletic type, larger breasts may interfere with your active routine. That’s because large implants can be literally heavy, may cause back problems, accelerate breast sagging, tissue thinning, and have higher visibility with the appearance of so-called double bubbles. [^39] These may then lead to a revision surgery to correct such problems.
You must also consider any plans of becoming pregnant in the future as it can affect your breast size. Losing or gaining weight is also a factor one should keep in mind when choosing the right size for herself. Meanwhile, implants come in a wide range of sizes. The higher the size number is, the bigger the implant.
Breast width and implant diameter
The width of your breasts is the distance between the inner and outer breast curves. The rule of thumb is, implants with moderate profile provide a natural look, high profile is for those with a narrow breast width, and low profile for those who prefer some volume on the breast edge, especially on the cleavage and upper breast area. Ideally, your implant diameter should be about the same as your breast width, if not slightly narrower.
For instance, a 12-centimeter breast width that is a match to an implant diameter of 11 to 12 centimeters will provide more satisfactory results. The diameter of your implants provides the outline of your breasts. Wider implants that are fitted to the body type tend to give upper fullness as well.
Mismatched breast implants can affect the overall breast aesthetic. An implant that’s too narrow may look like a ball inside a circle. On the other hand, too wide an implant can also affect the breast appearance and contribute to thinning of the breast tissue, which will make the implants more visible.
A simple and rough method when trying to find out your desired implant size is to try the implants on by inserting them inside your bra. Note that this will only give you an approximate visual on how your actual implants will appear beneath clothing. After breast augmentation, you may find that they look different inserted from when you tried them outside your breasts.
Breast tissue thickness
Breast tissue thickness is one of the factors to consider when choosing an implant size. There are instances when the breast width is wide, but the breast tissue is thin. Instead of a wide implant, choosing a narrow and moderate implant size would then be more appropriate.
When wide implants are used on patients with very thin breast tissue, it will tug the skin even more. This will lead to less padding over the implant, and may result in ripples. In this regard, even if the breast width is 12 centimeters, the implant diameter of 10.5 centimeters may be considered the right size.
Intra operative sizing
As the ultimate, last-minute size checking method, you can try two different implant sizes during the actual surgery. This is when you can’t decide on a single one, so at best, you are down to two choices. Once you have communicated your “breast wishes” to your surgeon, you leave it in his expert hands and eyes to try both implant sizes after the surgical creation of breast pockets, and allow him to decide which one will be permanently placed on you.
The deciding factor
There will be times when the doctor and patient will be in disagreement in terms of determining the implant size. So who decides then, is it the patient or the surgeon? Although it’s easy to say that the client is the decision-maker in this case, it can be a tricky aspect.
While responsible plastic surgeons will never fail to educate their patients to arm them with an informed decision, there have been some that will discourage those who believe in the “go big or go home” ideal by explaining the cons of implants that are deemed too large.
Although there is no correlation found between implant size and complications, [^42] having too big implants may not be the best option for the individual. However, patient surveys indicate an effect of implant size on the satisfaction ratings. [^37] In other words, women tend to favor larger implants to make them happy.
A related study indicated that more women had repeat surgeries after having 300- 350cc breast implants on their first operation compared to those who went for bigger implant sizes such as above 350cc. [^43] At the end of the day, the patient still has the final say.
The attending surgeon can only offer advice and discuss thoroughly what the patient must know beforehand. It is up to his discretion whether to follow the patient’s request, or refuse to take on the surgery.
Breast implant shapes
Aside from size, the shape of the breast implant is another important consideration. It is said that 15 percent of women who are thinking about undergoing breast surgery point to shape improvement as the reason for breast enhancement. [^38]
Should you go for the conventional round shape, or the teardrop type? While women may already have their own preferences, it is always a good idea to listen to what your doctor has to say about it.

Round breast implants
The most commonly used, round shape implants will produce a spherical appearance, with more fullness in the upper chest. These are optimal solutions to sagging problems, and for women who are going for a “busty” look. These implants are cheaper compared to other breast implant shapes.
Clients can count on round implants to give them bonus lift and cleavage. However, some women find breasts with such implants as looking too artificial. Having that round shape makes it symmetrical, and natural breasts don’t have a perfect symmetry.
As an advantage, implant rotation will not be a problem. It is also not as prone to wrinkling as a teardrop breast implant. As such, round implants may have fewer complications when compared to the shaped implant types.
Shaped breast implants
Shaped or anatomical breast implants veer away from the fixed round shape of conventional implants. The shape these implants often use is the teardrop form, which is thinner in the upper portion, and gradually gaining fullness downwards given their concentration at the bottom. They are often filled with silicone instead of saline in order to maintain its shape.
Considered the new gold standard in breast augmentation, gummy bear implants are made of dense cohesive silicone gel that aims to provide the natural contour and firmness of real breasts. As such, these aptly named breast implants are more equipped to delay gravity brought about by aging.
With its form-fitting structure, gummy bear implants are deemed safer options. Incidences of rippling, folding, and creasing are significantly diminished. As a result, medical complications from torn and leaking implants are much less.
In the right patient, especially those with mild sagging, teardrop implants are a great option. They may already provide sufficient elevation to the breasts, eradicating the need for a separate breast lift procedure.
Breast implant profiles
While it is common for patients to know the size, shape, type they want in a breast implant, they often don’t realize that implant profile is just as important. Breast implant profile consists of the projection, or how the breasts project forward from the chest wall while in a standing position.
It also includes the general silhouette of the implant, which represents the base diameter and volume. [^44] 250cc breast implants for example, can have different profiles because of the varying widths and projection.
There are usually 5 breast implant profiles, namely: low, moderate, moderate plus, high, and ultra high, and sometimes even more depending on the brand of the implant. Low profile implants are considerably flat and provide a minimal projection. They would usually fit body types that have wider chests. However, not many women prefer this option.

High profile implants on the other hand, tend to be very narrow at their base in order to achieve maximum projection. Needless to say, such implants have the fullest round shape. These may look unnatural on some patients, although they could work well with petite women.
Moderate profile implants are on that relatively sweet spot between low and high profile breast implants. They project more compared to the low profile, but less than the high profile type. These are deemed appropriate for narrower chests. Overall, the body proportions and expected results should be factored in when choosing the right implant profile.
It should be noted that the lack of standardized implant profiles across manufacturers may cause confusion and clinical errors. [^44] Therefore, discerning questions must be asked by the plastic surgeon, especially if the patient indicates a specific type of implant profile such as a “moderate-classic”, which could only be available in a particular implant brand.
Breast implant textures
There are two breast implants according to texture. The smooth type is consistent with a sleek surface compared to the textured implant, which has a rough feel. Both texture options have their own advantages and disadvantages which the patient should weigh before deciding on the final implant.

Smooth implants
Smooth breast implants are used more often in breast augmentation surgeries. They have a longer history, having been tested since the very first implants came out in the 60s. These implants can move in the breast pocket without drag. Their thinner skin has a softer feel and generally last longer.
Rippling in smooth implants is significantly reduced because of their smooth texture. However, they are more prone to malpositioning, which will require a breast revision surgery to fix.
Textured implants
These implants were developed to address the issue of capsular contracture, a complication brought about by the response of the immune system to a foreign body. [^45] This is where the body reacts by producing hardened scar tissue around the breast implant, which can result in irregular shape and asymmetry. It is presumed that its incidence is increased with the use of smooth implants, among other factors.
Textured implants possess a slight grainy roughness, which is believed to improve their adherence to the surrounding tissue. This way, the implants do not get displaced easily from their original position, especially if the teardrop shape is used.
Implant manufacturers have made their own texturing designs such as Natrelle’s “macrotexturing”, Mentor’s “microtexturing”, and the latest “nanotexturing” by Motiva Implants. [^46] However, textured breast implants tend to have ripples more which can lead to leakage. They are also expensive when compared to smooth implants.
It was observed that the use of textured breast implants can decrease the chances of capsular contracture. [^47] However, many argue this to be false, stating there is no remarkable difference of its occurrence on both smooth and textured implants. [^48] As such, more surgeons continue to use smooth implants on their patients.
Breast implant incision
An experienced and skillful surgeon comes to play when making incisions for your breast implant. The patient would normally prefer the resulting scars be as invisible and unnoticeable as possible. The surgeon may employ any of the following four incision methods, which may also depend on the client’s request and her body anatomy.
Transaxillary incision
This entails a small incision in the natural folds of the armpit where the breast implant will be placed either bluntly, or with the help of an endoscope. [^49] Afterwards, a breast channel and pocket will be created.
While both saline and medium size silicone implants can be inserted using this technique, it is saline that suits this incision best. This is because it can be placed inside with a small incision using an empty shell compared to a pre-filled silicone gel implant.
One of the clear advantages of transaxillary incision is the aesthetics. There will be no visible scarring on the breasts themselves. And because the incision is on the armpit folds, the scar is also less obvious.
This is also ideal if the patient plans to have children and perform breastfeeding in the future. With the incision made in the armpit, the mammary glands are less likely to be damaged in the process.
Performing a blunt procedure for this incision however, may cause some nerve damage. This can lead to numbness in the surrounding area. One study found that the risk of capsular contracture is higher for transaxillary incisions compared to other types. [^50]
In case of a revision or secondary surgery, it must be noted that the surgeon can no longer use the same incision location. It will also be difficult to achieve breast symmetry using this technique [^49] although it may help if your doctor is highly skillful.
Inframammary incision
This is the most common incision method practiced by surgeons despite the more visible scar that remains. [^51] Inframammary incisions are made in the lower breast fold resting on the chest wall. From a doctor’s point of view, it permits a good visual of the breast pockets to be made, facilitating the process. [^49]
This incision is created with up to two inches in size, which should be easily concealed by the breast crease. Although, a smaller incision at 1.7 centimeters is still possible if empty saline shells will be used as implants. [^51] Nonetheless, it may still leave a noticeable scar on the site.
In any case, this type of incision should then work well with those whose breasts hang below it as it’s a good way to hide it. The larger incision allows a better access point for a bigger implant and attain the desired pocket boundaries.
With its proximity to the surgery area, bleeding can be controlled and more precision can be achieved. The incision site can also be reopened should there be succeeding breast surgeries.
It is unlikely to have nerve damage in the nipple area with an inframammary incision. However, the scar on the breast fold can either move up or down in the event of further breast enhancement or reduction. For clients with a very small original breast size, they might need a highly skillful cosmetic surgeon that will execute the procedure using the type of incision that will be most suitable.
Periareolar incision
The periareolar incision is one that allows implants a direct access to the breast. It is usually located on the lower edge of the areola where its circle outline is. It allows usage of saline implants as well as moderate sized silicone implants, which can be possible with a larger incision.
Patients would prefer this type of incision because the scars can be nearly invisible given the pigmented skin of the areola. With the incision placed at the junction, the scar heals in such a way that it becomes imperceptible. [^52] This is also more likely to occur in women who have a considerable areola size that has a distinguished border.
For the surgeon, he has a clearer visual that allows controlled creation of the breast pocket. [^52] In the event of a revision surgery, the same incisions can be reopened without causing problems.
However, there are a few drawbacks to this incision method. The most common is the loss of nipple sensation, which happens more with smaller areolas. Several clinical studies point to the periareolar incision as having a higher rate of capsular contracture compared to other types of incision. [^53, 54]
If the client will be breastfeeding in the future, she might encounter some difficulty as it is possible that it can affect the milk ducts in the breast.
Transumbilical incision
Also called TUBA, transumbilical incisions have been proven safe for breast implantation. [^55] This approach involves the placement of the incision above the navel.
While it may be the most uncommon, TUBA is quite less invasive given that the abdomen has a higher elasticity among skin regions. Using an endoscope, a tunnel is created by cutting through the subcutaneous fat all the way to the breast area.

Aside from avoiding breast scars, the transumbilical incision requires less anesthesia and analgesics compared to other incision types because of the absence of tension on the incision itself. [^56]
With the use of inflatable implants, the formation of breast pockets through expansion eliminates extra space where otherwise, infection could thrive. Another benefit for this type of remote incision is the immediate observation of the final breast shape after implantation.
Transumbilical incisions however, cannot accommodate prefilled implants such as silicone gel, structured and gummy bear implants. As this is no easy method, it takes highly intensive training and specialized equipment to perform this procedure.
It leaves very little room for error, hence only a few skillful plastic surgeons employ this technique. Just like with transaxillary incisions, transumbilical site cannot be reopened during a revision surgery.
Breast implant placement
Which method is best – over the muscle, or below it? Roughly speaking, these two options will be presented to the client. Each individual has her own unique characteristics such that there is no best answer to this question.
The positioning of implants will largely depend on the woman’s physique and how good they can look on her. There are several breast implant placements that should be decided both by the surgeon and the patient.
Subglandular technique
Also called “over the muscle” placement, the subglandular technique is one of the main surgical planes in breast augmentation. This is where the implant is lodged between the pectoralis major muscle and the mammary gland. It is deemed by many doctors as representing a more natural surface which produces realistic-looking breasts. [^57]
Placing implants in this plane can correct mild breast ptosis, or sagging, which would otherwise require a separate procedure that involves lifting the nipples and areola. [^58] It can also be suggested for those with tubular breast deformities. When you are physically active, the implants are not affected by the pectoralis muscle movement. From a surgeon’s standpoint, the subglandular technique makes for easier dissection.
On the other hand, this type of implant placement will not suit women with thin breast tissue. This is because it will make the breast implants practically visible, including the rippling and wrinkling. Thus, it can produce a more “surgically done” or “bubble-like” look.
According to many radiologists, placing your breast implants above the muscle interferes with mammography testing. Moreover, it has been observed that capsular contracture is more likely to occur when this type of implant placement is employed. [^45]
Subfascial technique
Breast augmentation using the subfascial technique also places the implant above the muscle. Its difference from the subglandular method is its placement behind the fascia, [^59] which is a very thin membrane covering the muscle. Somehow, this layer can provide a slight padding to the implant, which will help provide a more natural appearance to the breasts.
The visibility of the implant outline is decreased except for an extremely thin patient. [^59] The implant supposedly sustains its position much better in this method. This also prevents several issues brought about by placing the breast implants beneath the muscle.
One of the benefits of this implant placement is improved cleavage. It also possesses the advantages similar to subglandular placement such as a bonus breast lift and less pain post surgery. A clinical study has concluded that this placement offers better breast aesthetics, with the optimized dynamics of both the implant and surrounding breast tissue. [^60]
Subpectoral technique
This technique belongs to the “under the muscle” category. With the subpectoral approach, the breast pocket is created by lifting the pectoralis major muscle of the chest where the implant will be placed. With the help of a mesh, it forms an internal bra that will hold the breast implant. [^61]
Technically speaking, the entire implant is not behind the muscle, only the upper portion is. That’s because when the pectoralis major muscle is surgically modified, it only covers the upper half of the implant while the lower half is submammary or beneath the breast tissue. [^62] This becomes crucial in the final appearance of the breasts as the implants are concealed at the upper pole where they need it the most.
In the meantime, it is crucial for the surgeon to retract the minor muscle upwards across the lower part of the breast. Otherwise, the breasts will have a bizarre appearance and create an awkward implant animation where the breast implant moves around with arm movement during muscle contraction. [^57]
While the subpectoral placement may reduce risks of capsular contractures and implant visibility, recovery time usually takes longer and will likely feel more painful. As such, the breast implants may take awhile to settle in their natural position post surgery.
Submuscular technique
This is a bonafide example of an “under the muscle”approach where the breast implant is placed behind the pectoralis major muscle, supporting fascia or connective tissue, and non pectoral muscle groups. It results in less palpable implants and lower incidence of capsular contracture.
Placing implants this way are best for mammograms as well because the breast tissue can be fully examined without their presence.
Submuscular placement is usually recommended for very lean women as the muscle is able to hide the implant outline and rippling if any. [^63] It is also ideal when using gummy bear implants which are firmer than normal silicone implants. When performed in conjunction with a breast lift, it helps improve the blood supply to the breasts.
One of the main issues of this technique however, is the implant animation that’s why this is no longer employed as much in breast augmentation surgery. A study was conducted on the waterfall effect which looks like sliding breast tissue over an implant which happens often with submuscular breast pockets. [^64] Surgeons who take the “under the muscle” route would instead choose subpectoral, or dual plane technique.
Prepectoral technique
Performed in breast reconstruction, prepectoral implant placement involves positioning the implants on top of the pectoralis major muscle. They are then supported by a mesh called acellular dermal matrix or ADM.
Patients are said to benefit more from this method by having less pain post surgery, avoid implant animation, decreased rate of capsular contracture and higher patient satisfaction. It even preserves the viability of the pectoralis major muscle and chest wall. [^65]
Dual plane technique
This implant placement may be similar to the subpectoral technique and its effect on breast shape. [^66] Dual plane was designed to combine submammary and partial subpectoral pocket locations to get the most out of each while limiting the risks of having just one. [^67]
This method is considered more as a deep plane rather than a dual one. The reason behind this is, there is only one plane inhabited by the implant in actuality. It starts from one tissue and continues to another, hence the dual plane label. [^62]
The difference from the subpectoral placement is its inclusion of a partial prepectoral dissection that enhances breast shape and lifts the nipple.
Breast Implant Safety: Risks and Side Effects
There have been numerous studies in the past 5 decades of clinical application that show the efficacy of augmentation mammaplasty. When performed correctly, breast augmentation using implants is a relatively safe procedure, with an estimated more than 5 million women in the US having silicone breast implants to date.
Being artificial devices however, silicone implants have a failure rate and may require surgical maintenance for some patients. [^68]
The straight safety facts:
1) Breast implants do not cause breast cancer
A common misconception, breast implants neither lead to nor aggravate breast cancer, or any major disease. [^69] On the contrary, those with breast implants are said to have a lesser risk for cancer according to a number of studies. [^68]
2) Breast implants do not taint breast milk
There is no evidence that suggests an increased level of silicone in breast milk of women who have breast implants.
3) Breast implants are not dangerous to an unborn child
Silicone does not migrate to the placenta where it can affect a developing fetus.
4) Breast implants do not interfere with radiation treatment
Despite a few published reports, there is no sufficient evidence that says implants diminish the efficacy of radiation. In the same manner, radiation does not affect the implants either, although more studies are needed to establish its link to capsular contracture.
5) Breast implant technology makes it safer today
Many changes have been implemented since the start of silicone implant use. There are a number of methodologies that decrease its risks of complications, with more innovations in the pipeline. Currently, many implant shells have been fortified to prevent seepage and rupture.
6) Breast implants do not mess with immunity
While the body reacts to the presence of an antigen, which is a protein found in bacteria and viruses, it has not been proven that silicone implants trigger this mechanism.
Like many surgical operations, breast augmentation with the use of implants, has accompanying risks that range from minor to life-threatening. It has been found that most complications would usually arise from those with silicone gel implants than saline implants.
Up to 40 percent of women who have undergone breast reconstruction can expect at least one of its adverse effects. [^69]
Capsular contracture is perhaps one of the most feared side effects of breast augmentation. A fibrous tissue capsule forms around the implant as the body’s extreme reaction to a foreign agent. This will require major surgery in order to remove the implant and break down the tissue overgrowth.
Other side effects (but are not limited to) include:
Implant rupture – This is when the silicone gel or saline solution escapes the shell of the implant. It is usually caused by accidental needle pricks during stitching of the incision, flaws on the shell itself, overfilling in the case of saline implants, or when the breast is severely compressed. Over time, the implant can also weaken which can lead to its deflation.
Scarring – This is often the reason why some women will insist on a remote incision so that there will be no scars on their breast mound. Age, incision size, and skin color can affect how your scars will appear.
Implant displacement – Breast implants can shift in another direction at any point in time. They could move towards the armpit, bottom out, ride too high up your chest, or form a tenting called symmastia (a.k.a. uniboob).
Infection – Most surgeries, if not all, carry the risk of infection, which may develop in the surgery area. Some local infections can be treated with antibiotics such as staph. At its worst form, an infection can even trigger a severe capsular contracture.
Hematoma – Surgeons manage this by using drains post surgery in order to manage bleeding and prevent the blood from collecting around the implants.
Breast pain – When there is persistent pain after the surgery, this would usually prompt an implant replacement, if not its removal.
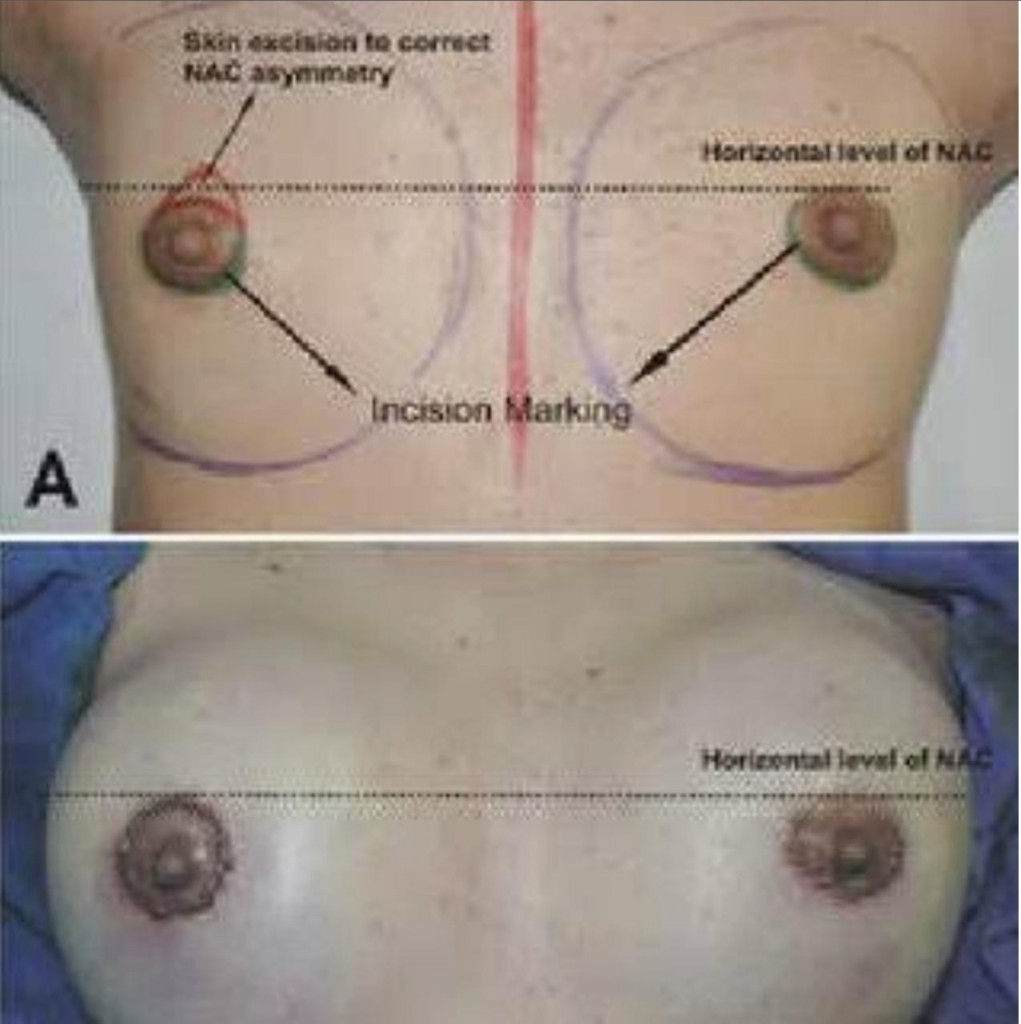
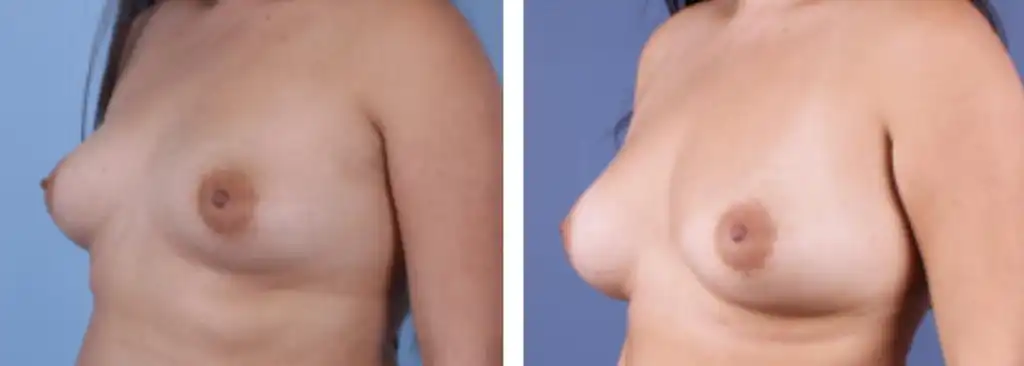
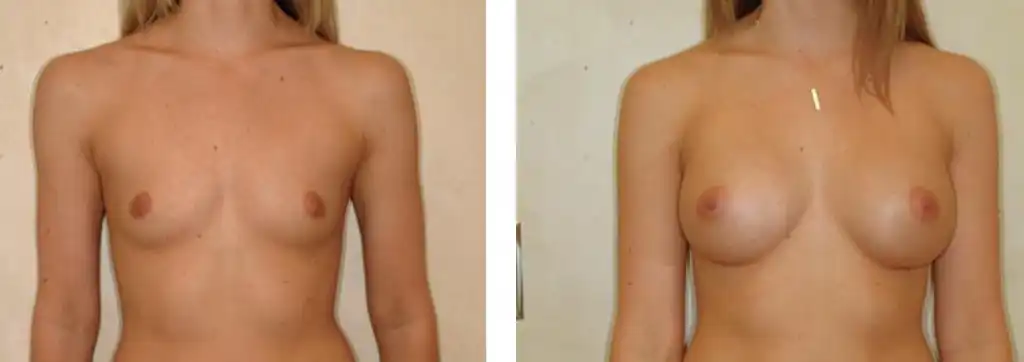
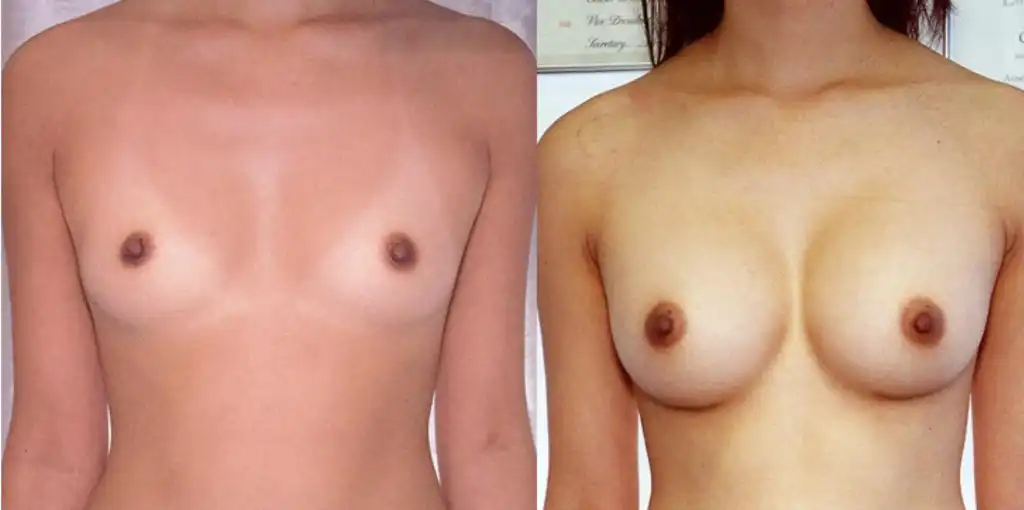
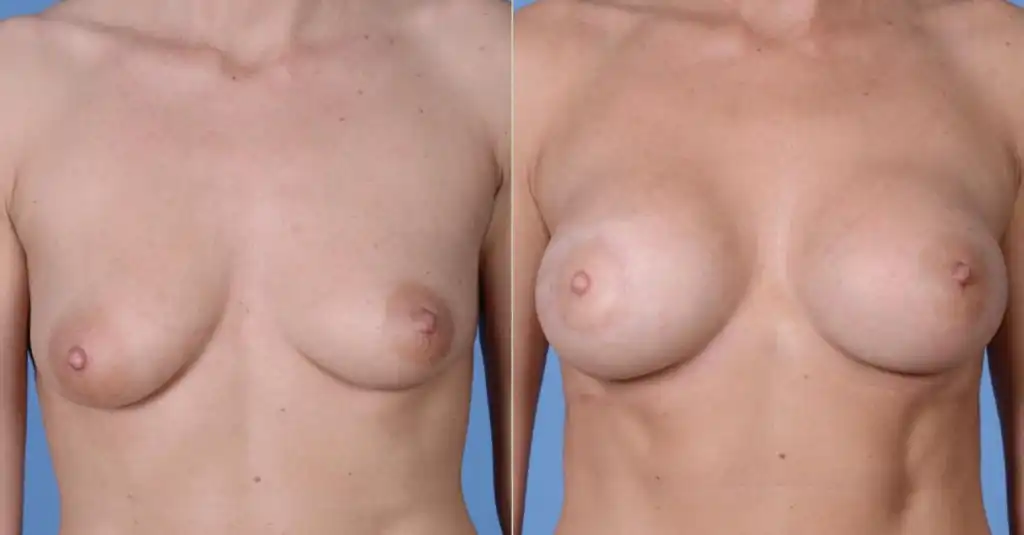
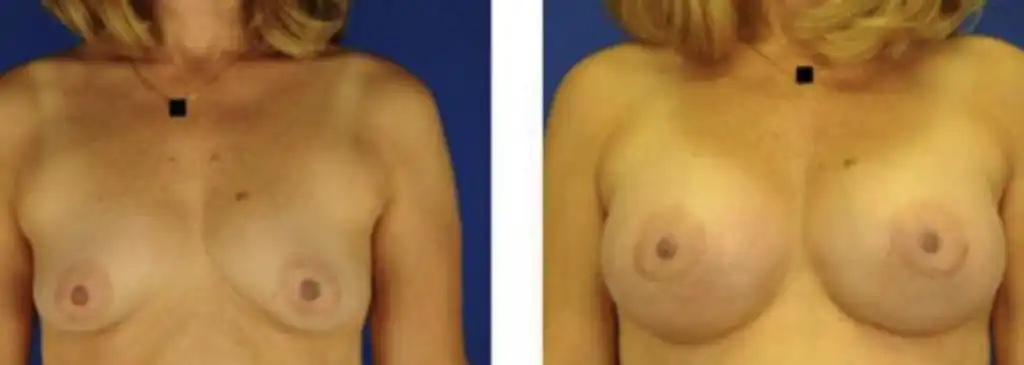
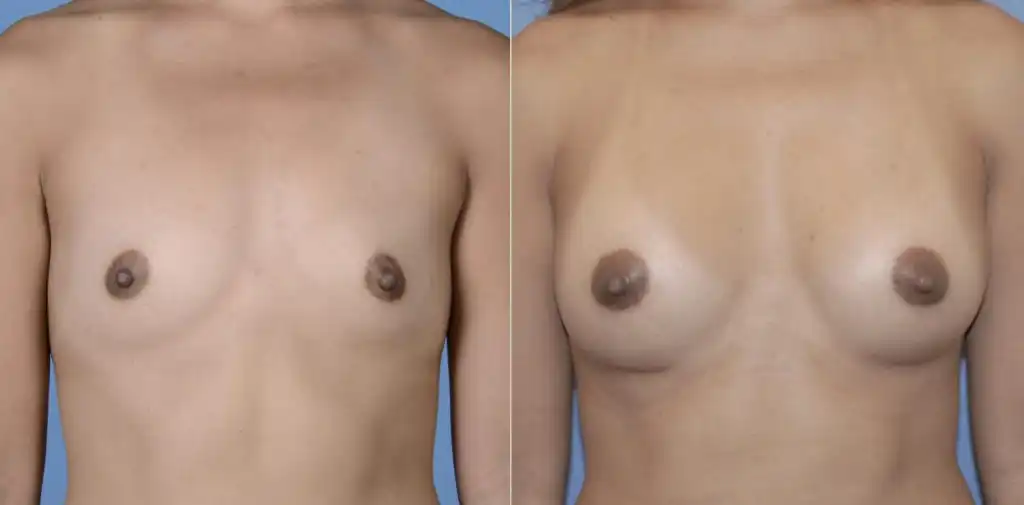
Breast Augmentation Before and After Photos









FAQs
How do I know if I’m a good candidate for breast augmentation?
If you are dissatisfied with the size, shape, symmetry, or firmness of your breasts, you may consider breast augmentation surgery. That is if you are generally healthy and have realistic expectations.
Although there is a high satisfaction rate among patients after a successful breast surgery, you cannot expect to achieve perfection more than significant improvement on your breasts.
Needless to say, you do not qualify if you are pregnant, breastfeeding, have existing cancer or severe illness, and below the age requirement according to the type of implant you prefer.
How much does the Breast Augmentation Surgery Cost?
As mentioned in the article, silicone implants are more expensive than saline ones, with the shaped types priced higher than round implants. The average cost of breast augmentation surgery is on average $4,000 which may already include fees of the surgeon, anesthesia, facility use, medical tests, prescriptions, and post surgical care paraphernalia.
However, prices may differ significantly depending on the doctor and region such that, silicone implants may cost $2,000 more in New York than say, in Texas. Usually, if the surgeon is a celebrity in his own right, he can charge as much as $10,000 a pop. You can always get a quotation during your consult so you can set a budget for it if necessary.
What should I look for when choosing a surgeon?
It is crucial to find a surgeon who is both licensed and affiliated with a professional plastic surgery association. In the US, the doctor should have a certification with either American Board of Cosmetic Surgery, or American Society of Plastic Surgeons.
He must also have extensive training and experience with breast augmentation, and holds clinic in an accredited medical facility. His medical team should be comprised of licensed professionals like nurses and anesthesiologists.
Referrals are also great options, but don’t forget to check for credentials and board certification regardless. To facilitate your post surgical checkups, it is highly advisable to pick a doctor that is easily accessible or near your place of residence.
Lastly, it’s important that you feel confident and comfortable with the doctor of your choice. You can gauge this when you schedule a consultation where you can have the opportunity not only to ask about surgery questions, but also to get to know your surgeon. While you’re at it, you can even check any of his social media accounts for further validation.
What is the recovery process like?
Given the modern techniques used in breast augmentations, recovery time has been much faster than ever. You can practically go back to work after 2 days of full rest following the procedure. As there will be swelling, bruising, and soreness, you will be advised to take it slow for several days.
You will be visiting your doctor for checkups during which he will recommend breast massage techniques that will help prevent capsular contracture. Your breasts will continue to be swollen for a month or more, and expect total recovery 2 months after surgery, more or less. Until then, you will not engage in any strenuous activity such as workouts, heavy lifting, and the like.
Immediately after the surgery, your breasts and nipple may feel numb and you may be instructed to wear a surgical bra. Your chest area may also feel tight as it adjusts to the presence of the implants.
While you will be allowed to take a shower a day after, you will be asked to refrain from swimming or anything that lets you soak in still water for 2 weeks. Surgical dressing may be regularly replaced up to seven days.
How should I prepare for the surgery?
Aside from proper diet and regular exercise, it is recommended that each patient who is about to undergo breast augmentation observes the following guidelines prior surgery:
- Advise your attending surgeon about any medication you are taking as some of them may affect your eligibility to do the operation.
- Refrain from alcohol intake at least a week before.
- Stop smoking one month prior.
- Avoid exposure to sick people.
- Do the necessary post surgery arrangements, such as transportation, vacation leave from work, having a companion, non-wired bras, immediate kit consisting of your ice packs, vitamins, and prescriptions.
- Take a shower right before the operation, but don’t use makeup, lotion, antiperspirant and other toiletries.
- You must remove all types of jewelry before you embark on the operation.
- Wear something loose fitting on the day of the surgery.
- Do not take anything solid 8 hours before while drinking anything is not allowed within 4 hours leading to the surgery.
How do I book an appointment?
As soon as you have narrowed down your list of preferred doctors, you should set an appointment to discuss every aspect of your intended breast surgery in great detail. This will help you arrive at a final decision whether to proceed with it through that surgeon or not.
Any professional doctor will always give you enough time to decide before committing to the surgery. Whatever the case may be, you can book your appointment by visiting VitalBar. Our PlasticSpot booking system is perfect for finding the most suitable plastic surgeon near you. You can make bookings through our own city pages if you are in Vancouver or Calgary. Plastic surgery operations including breast augmentation are welcome.
Summary
Breast augmentation can bring immediate gratification to the patient, especially if she has realistic goals to begin with. Ideally speaking, it’s always safer to stay conservative in picking an implant size rather than opt for 3 or 4 cups bigger right away. Any responsible doctor will say the same thing.
You must realize that whatever the size you choose impacts you long term. The highly skilled and professional doctors at VitalBar will help you through this process in order for you to make that wise choice. They are dedicated to providing you with the results you desire. At the end of the day, the decision is yours to make.
References:
[^1]: Anonymous. Year-to-year comparisons: 2017 vs 2016. ISAPS. 2018
[^2]: Ross, A. 2017 Cosmetic Surgery Age Distribution. ASPS. 2018
[^3]: Pensler, JM. Submuscular Breast Augmentation. Medscape. 2017
[^4]: Champaneria, M. et al. The Evolution of Breast Reconstruction: A Historical Perspective. World Journal of Surg. 2012
[^5]: Peters, W. Fornasier, V. Complications from injectable materials used for breast augmentation. Can J Plast Surg. 2009
[^6]: Pfleiderer, B. Garrido, L. Migration and accumulation of silicone in the liver of women with silicone gel-filled breast implants. Magn Reson Med. 1995
[^7]: Peters, W. The evolution of breast implants. Can J Plast Surg. 2002
[^8]: Maxwell, GP. Gabriel, A. Possible future development of implants and breast augmentation. Clin Plast Surg. 2009
[^9]: Romm, S. The Changing Face of Beauty. Toronto: Mosby Year Book. 1992
[^10]: Maxwell, GP. Gabriel, A. Breast implant design. Gland Surg. 2017
[^11]: Maxwell, GP. Gabriel, A. The evolution of breast implants. Clin Plast Surg. 2009
[^12]: Anonymous. Breast Implant-Associated Anaplastic Large Cell Lymphoma (BIA-ALCL). FDA. 2019
[^13]: Goodman, CM. The life span of silicone gel breast implants and a comparison of mammography, ultrasonography, and magnetic resonance imaging in detecting implant rupture: a meta-analysis. Ann Plast Surg. 1998
[^14]: Anonymous. Types of Breast Implants. FDA. 2019
[^15]: Spear, SL. Jespersen, MR. Breast Implants: Saline or Silicone? Aesthetic Surg Jour. 2010
[^16]: Horton, K. Silicone vs saline breast implants. ASPS. 2017
[^17]: Nichter, LS. et al. IDEAL IMPLANT Structured Breast Implants
Core Study Results at 6 Years. Plastic and Recon Surg. 2018
[^18]: Bircoll M. Cosmetic breast augmentation utilizing autologous fat and liposuction techniques. Plast Reconstr Surg. 1987
[^19]: Kasem, A. et al. Breast Lipofilling: A Review of Current Practice. Arch Plast Surg. 2015
[^20]: Coleman, SR. Fat grafting to the breast revisited: safety and efficacy. Plast Reconstr Surg. 2007
[^21]:Coleman SR. Hand rejuvenation with structural fat grafting. Plast Reconstr Surg. 2002
[^22]: Rohrich RJ, Sorokin ES, Brown SA. In search of improved fat transfer viability: a quantitative analysis of the role of centrifugation and harvest site. Plast Reconstr Surg. 2004
[^23]: Moyer HR, Ghazi B, Saunders N, et al. Contamination in smooth gel breast implant placement: testing a funnel versus digital insertion technique in a cadaver model. Aesthet Surg J. 2012
[^24]: Newman, AN. et al. Effect of Keller Funnel on the Rate of Capsular Contracture in Periareolar Breast Augmentation. Plastic and Reconstructive Surg. 2018
[^25]: Wiener, TC. Relationship of incision choice to capsular contracture. Aesthetic Plast Surg. 2008
[^26]: Flugstad, NA. et al. Does Implant Insertion with a Funnel Decrease Capsular Contracture? A Preliminary Report. Aesthetic Plast Surg. 2016
[^27]: Guyomard, V. et al. Systematic review of studies of patients’ satisfaction with breast reconstruction after mastectomy. Breast. 2007
[^28]: Mesbahi, AN. et al. Breast reconstruction with prosthetic implants. Cancer Journal, 2008
[^29]: Regan, JP, Schaffner, AD. Breast Reconstruction Expander Implant. StatPearls. 2017
[^30]: Bellini, E. et al. Two-Stage Tissue-Expander Breast Reconstruction: A Focus on the Surgical Technique. BioMed Research Intl. 2017
[^31]: Spear SL, Pelletiere, Majidian, A. Immediate breast reconstruction in two stages using textured, integrated-valve tissue expanders and breast implants: A retrospective review of 171 consecutive breast reconstructions from 1989 to 1996. Plastic and Recon Surg. 1998
[^32]: Demiri, E. et al. Becker Expander-Based Breast Reconstruction Following Wise Pattern Skin-Reducing Mastectomy: Complication Rates and Risk Factors. Aesthetic Plastic Surgery, 2017
[^33]: Whidden, PG. Simultaneous breast augmentation and mastopexy. Can J Plast Surg. 2003
[^34]: Benelli LC. A new periareolar mammoplasty: The “Round Block” Technique. Aesthetic Plast Surg. 1990
[^35]: Sterodimas, A. et al. Ethical issues in plastic and reconstructive surgery (review). Aesthetic Plast Surg. 2011
[^36]: Lev, AI. Transgender emergence: guidelines for workingwith gender-variant people and their families. Haworth Press. 2004
[^37]: Swanson, E. Prospective outcome study of 225 cases of breast augmentation. Plast Reconstr Surg. 2013
[^38]: Nava, MB. A decision-making method for breast augmentation based on 25 years of practice. Arch Plast Surg. 2018
[^39]: Mallucci, P. Branford, OA. Reply: design for natural breast augmentation: the ICE principle. Plast Reconstr Surg. 2017
[^40]: Tebbetts, JB. The greatest myths in breast augmentation. Plast Reconstr Surg. 2001
[^41]: Adams, WP. Jr. The process of breast augmentation: Four sequential steps for optimizing outcomes for patients. Plast Reconstr Surg. 2008
[^42]: Swanson, E. Prospective comparative clinical evaluation of 784 consecutive cases of breast augmentation and vertical mammaplasty, performed individually and in combination. Plast Reconstr Surg. 2013
[^43]: Huang, GJ. et al. Transaxillary subpectoral augmentation mammaplasty: a single surgeon’s 20-year experience. Aesthet Surg J. 2011
[^44]: Wan, D. Rohrich, R. Making Sense of Implant “Profile” in Breast Augmentation. Plastic Recon Surg. 2017
[^45]: Headon, H. et al. Capsular Contracture after Breast Augmentation: An Update for Clinical Practice. Arch Plast Surg. 2015
[^46]: Abramo, AC. et al. How texture-inducing contraction vectors affect the fibrous capsule shrinkage around breasts implants? Aesthetic Plast Surg. 2010
[^47]: Pollock, H. Breast capsular contracture: a retrospective study of textured versus smooth silicone implants. Plast Reconstr Surg. 1993
[^48]: Becker, H. Springer, R. Prevention of capsular contracture. Plast Reconstr Surg. 1999
[^49]: Ramachandran, K. Breast augmentation. Indian Journal Plast Surg. 2008
[^50]: Jacobson, JM. Effect of Incision Choice on Outcomes in Primary Breast Augmentation. Aesthetic Surg Jour. 2012
[^51]: Fanous, N. et al. Minimal inframammary incision for breast augmentation. Can J Plast Surg. 2008
[^52]: Mohmand, MH. Periareolar Extra-Glandular Breast Augmentation. World J Plast Surg. 2013
[^53]: Li, S. et al. Capsular Contracture Rate After Breast Augmentation with Periareolar Versus Other Two (Inframammary and Transaxillary) Incisions: A Meta-Analysis. Aesthetic Plast Surg. 2018
[^54]: Wiener, TC. Relationship of incision choice to capsular contracture. Aesthetic Plast Surg. 2008
[^55]: Dowden R V. Why the transumbilical breast augmentation is safe for implants. Plast Reconstr Surg. 2002
[^56]: Dowden, RV. Transumbilical Breast Augmentation Is Safe and Effective. Semin Plast Surg. 2008
[^57]: Lesavoy, MA. et al. Difficulties with subpectoral augmentation mammaplasty and its correction: the role of subglandular site change in revision aesthetic breast surgery. Plastic Reconstr Surg. 2010
[^58]: Shridharani, SM. et al. Breast augmentation. Eplasty. 2013
[^59]: Hunstad, JP. Webb, LS. Subfascial breast augmentation: a comprehensive experience. Aesthetic Plast Surg. 2010
[^60]: Siclovan, HR. Jomah, JA. Advantages and outcomes in subfascial breast augmentation: a two-year review of experience. Aesthetic Plast Surg. 2008
[^61]: Vidya, R. et al. Management based on grading of animation deformity following implant-based subpectoral breast reconstruction. Arch Plast Surg. 2018
[^62]: Swanson, E. Dual Plane versus Subpectoral Breast Augmentation: Is There a Difference? Plast Reconstr Surg Glob Open. 2016
[^63]: Hendricks, H. Complete submuscular breast augmentation: 650 cases managed using an alternative surgical technique. Aesthetic Plast Surg. 2007
[^64]: Frame, J. The waterfall effect in breast augmentation. Gland Surg. 2017
[^65]: Rebowe, RE. et al. The Evolution from Subcutaneous to Prepectoral Prosthetic Breast Reconstruction. Plast Reconstr Surg Glob Open. 2018
[^66]: Hidalgo, DA. Sinno, S. Current trends and controversies in breast augmentation. Plast Reconstr Surg. 2016
[^67]: Tebbets, JB. Dual plane breast augmentation: optimizing implant-soft-tissue relationships in a wide range of breast types. Plast Reconstr Surg. 2001
[^68]: Brody, GS. Silicone Breast Implant Safety and Efficacy. Medscape. 2017
[^69]: Grigg, M. et al. Information for Women About the Safety of Silicone Breast Implants. National Academy of Sciences. 2000